
PCOS Is Being Renamed PMOS. Here Is Why It Matters and What Every Woman Deserves to Know.
For years, women with irregular periods, acne, weight changes, facial hair growth, infertility, insulin resistance, and metabolic dysfunction have been handed a diagnosis built around the wrong organ.
Polycystic Ovarian Syndrome. PCOS.
Except that many of these women never had ovarian cysts at all.
This diagnostic mismatch is not a minor semantic issue. It has shaped how the condition is researched, how physicians are trained to recognize it, which specialists are expected to manage it, and most consequentially, how millions of women have been evaluated, treated, and dismissed for decades. The name has been part of the harm.
On May 12, 2026, an international consortium of researchers and physicians officially renamed PCOS to Polyendocrine Metabolic Ovarian Syndrome, or PMOS. This is one of the most significant reframings in women's medicine in a generation. Understanding why requires understanding what this condition actually is at a physiologic level, and why naming it after ovarian cysts was never scientifically accurate.
What PMOS Actually Is
PMOS is not an ovarian condition. It is a complex, multisystem, hormonal and metabolic syndrome driven by dysfunction across the endocrine, metabolic, and nervous systems simultaneously. The ovaries are involved, but they are responding to upstream signals rather than generating the problem themselves.
The condition affects between 8 and 13 percent of women of reproductive age worldwide, making it one of the most common endocrine disorders in women. Yet despite its prevalence, the average woman with PMOS sees multiple specialists over several years before receiving an accurate diagnosis. The referral loop is predictable and exhausting: gynecology sends her to endocrinology, endocrinology sends her back to gynecology, and the metabolic drivers at the root of her symptoms go unaddressed throughout.
This happens because the name directs clinical attention to the wrong place.
The HPA Axis: The Upstream Driver Most Physicians Miss
To understand PMOS, you have to understand the hypothalamic-pituitary-adrenal axis and its relationship to the hypothalamic-pituitary-ovarian axis. These two systems are deeply interconnected, and dysfunction in one reliably dysregulates the other.
In PMOS, the hypothalamus releases gonadotropin-releasing hormone, GnRH, at an abnormally high pulse frequency. This drives excess luteinizing hormone, LH, relative to follicle-stimulating hormone, FSH, from the pituitary. The resulting elevated LH to FSH ratio signals the ovarian theca cells to overproduce androgens, specifically testosterone and androstenedione, while simultaneously impairing follicular maturation and ovulation.
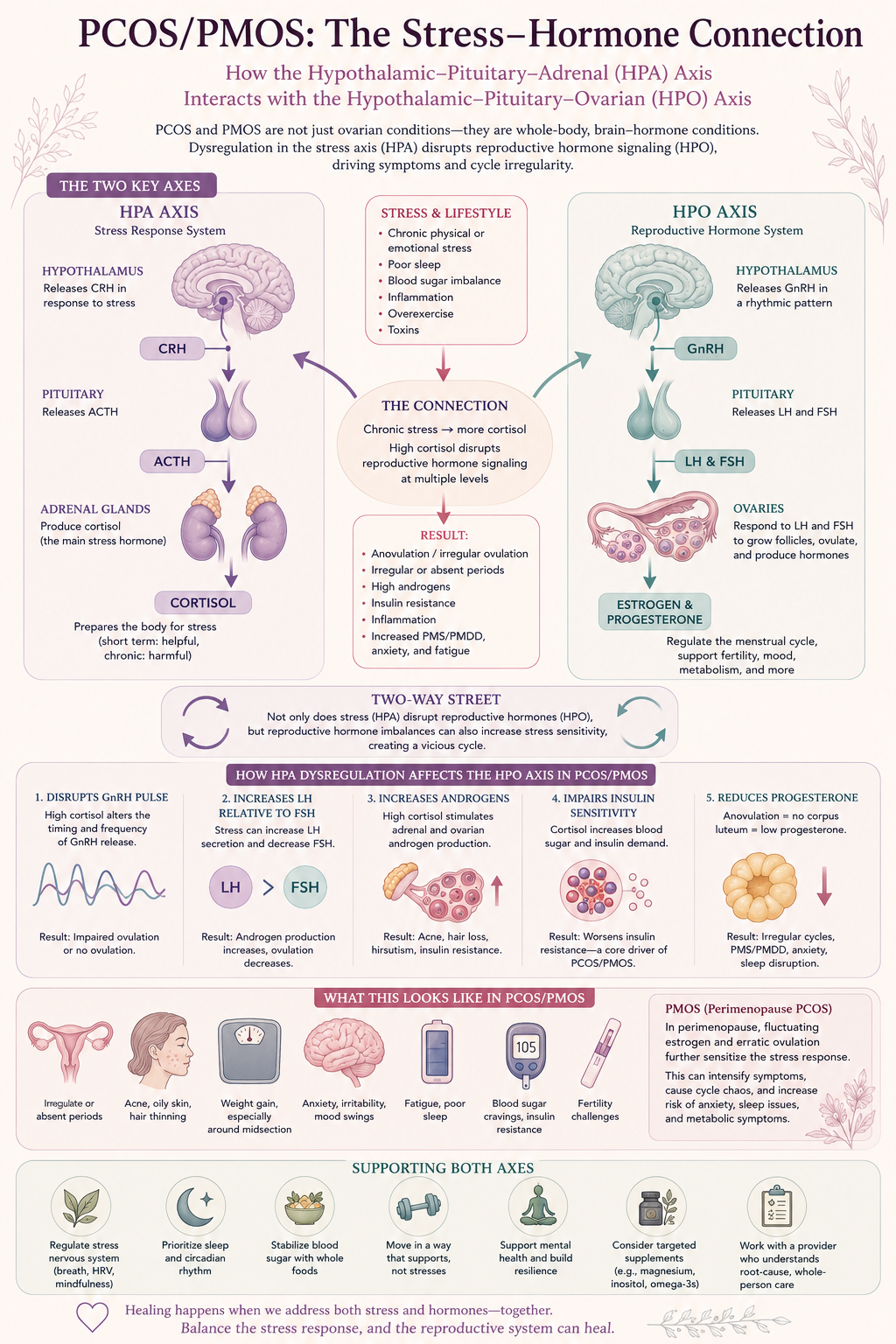
The relationship between the hypothalamic-pituitary-adrenal axis and hypothalamic-pituitary-ovarian axis in PCOS, now named PMOS, showing how stress, cortisol, insulin resistance, ovulation dysfunction, and hormone imbalance interact in women’s reproductive and metabolic health.
But the hypothalamus does not operate in isolation. Chronic stress, sleep disruption, and dysregulated cortisol output from the adrenal glands feed directly into hypothalamic signaling. Elevated cortisol promotes insulin resistance, and insulin resistance directly amplifies ovarian androgen production by stimulating theca cell activity. Hyperinsulinemia also suppresses sex hormone-binding globulin (SHBG, which increases the amount of free, biologically active testosterone circulating in the body.
The result is a self-reinforcing cycle. Elevated androgens disrupt sleep and increase stress reactivity. Disrupted sleep elevates cortisol. Elevated cortisol worsens insulin resistance. Insulin resistance drives more androgen production. The ovaries are not initiating this cascade. They are caught inside it.
This is why treating PMOS with birth control pills alone, which suppresses ovarian androgen production without addressing insulin resistance, cortisol dysregulation, or HPA axis dysfunction, produces symptomatic relief without resolving the underlying physiology. Symptoms return when the pill is discontinued because the metabolic drivers were never addressed.
This is also why adrenal androgens matter in this picture. In a meaningful subset of women with PMOS, elevated DHEAS indicates adrenal androgen excess alongside or instead of ovarian androgen excess. These women may not respond to ovarian-focused treatments at all. Distinguishing adrenal from ovarian androgen sources is a critical diagnostic step that is frequently skipped.
Cardiovascular and Inflammatory Risk: What the Research Shows
PMOS carries a cardiovascular risk profile that is significantly underappreciated in clinical practice, in part because the condition has historically been framed as a reproductive issue affecting young women rather than a lifelong metabolic syndrome requiring long-term cardiovascular surveillance.
The data are unambiguous and warrant serious clinical attention.
Women with PMOS have two to three times the risk of developing type 2 diabetes compared to women without the condition. Impaired glucose tolerance is present in approximately 35 percent of women with PMOS, and overt type 2 diabetes develops in up to 10 percent by their fourth decade. The insulin resistance driving these outcomes is present in 65 to 70 percent of women with PMOS regardless of body weight, which means lean women with PMOS carry the same metabolic risk as those with higher body mass index, a fact that is routinely missed when clinical assessment relies on weight as a proxy for metabolic health.
Cardiovascular risk markers are consistently elevated in women with PMOS. Studies demonstrate higher rates of hypertension, dyslipidemia, elevated triglycerides, reduced HDL cholesterol, and increased LDL particle size and oxidative modification. Subclinical atherosclerosis, measured by carotid intima-media thickness, is increased in women with PMOS across multiple studies, including in adolescents and young women. Endothelial dysfunction, an early and independent predictor of cardiovascular events, has been consistently documented.
The inflammatory picture is equally significant. Women with PMOS show elevated high-sensitivity C-reactive protein, increased oxidative stress markers, elevated interleukin-6 and tumor necrosis factor-alpha, and dysregulated adipokine signaling, including elevated leptin and reduced adiponectin. This chronic low-grade inflammatory state is not simply a consequence of metabolic dysfunction. It actively worsens insulin resistance, amplifies androgen production, and impairs ovarian function, creating a bidirectional inflammatory and hormonal feedback loop.
Sleep apnea, which itself drives systemic inflammation, insulin resistance, and HPA axis dysregulation, is present in women with PMOS at rates 5 to 30 times higher than in women without the condition, even after controlling for body weight. This association is dramatically underrecognized and underscreened in clinical practice.
Hidradenitis suppurativa, a chronic inflammatory skin condition affecting the apocrine gland-bearing areas, occurs at significantly higher rates in women with PMOS and shares overlapping pathophysiology including hyperandrogenism and systemic inflammation. Psychiatric comorbidities, including depression, anxiety, and disordered eating, are present at rates two to three times higher than in the general population, driven by a combination of hormonal dysregulation, chronic inflammation, and the profound psychological burden of living with a misunderstood and frequently dismissed condition.
The lifetime cardiovascular risk for women with PMOS is substantially elevated. This is not a condition that resolves after reproductive years. It is a lifelong metabolic syndrome that requires proactive surveillance and intervention across the lifespan.
Diagnosis: What a Complete Evaluation Actually Looks Like
A thorough evaluation for PMOS goes well beyond a pelvic ultrasound and a testosterone level. Clinicians practicing integrative and functional medicine approach this condition with a comprehensive laboratory and clinical assessment that reflects its systemic nature.
Hormonal assessment should include total and free testosterone, DHEAS to evaluate adrenal androgen contribution, LH and FSH with attention to the LH to FSH ratio, estradiol, progesterone, prolactin to rule out other causes of cycle irregularity, and thyroid function including TSH, free T3, and thyroid antibodies given the high co-occurrence of autoimmune thyroid disease in this population.
Metabolic assessment should include fasting glucose and insulin with calculation of HOMA-IR as a sensitive measure of insulin resistance, hemoglobin A1c, a fasting lipid panel with attention to triglycerides and HDL, and uric acid, which is elevated in insulin resistance and carries independent cardiovascular risk. A two-hour oral glucose tolerance test is the most sensitive tool for identifying impaired glucose tolerance and should be offered to all women with suspected PMOS rather than fasting glucose alone.
Inflammatory markers, including high-sensitivity CRP, homocysteine, and ferritin, provide important context for the inflammatory burden the patient is carrying. Assessment of sleep quality and screening for sleep apnea should be routine. Evaluation of cortisol and adrenal function is warranted when clinical presentation suggests significant HPA axis involvement, including history of chronic stress, trauma, burnout, or atypical androgen patterns.
Treatment: A Whole-System Approach
Effective treatment of PMOS requires addressing the root drivers rather than managing downstream symptoms in isolation. The following represents a comprehensive, evidence-informed approach that extends well beyond the historically narrow metformin-and-pill framework.
Insulin sensitization
Addressing insulin resistance is the cornerstone of metabolic treatment in PMOS. Metformin remains a useful tool in this category, particularly for women with significant insulin resistance or impaired glucose tolerance. However, it is one option within a broader landscape.
Inositol, specifically the combination of myo-inositol and D-chiro-inositol in a physiologic 40 to 1 ratio, has robust evidence supporting its use in PMOS. It improves insulin sensitivity, reduces androgen levels, restores ovulatory function, and improves oocyte quality. It is well tolerated, widely available, and should be considered a first-line nutritional intervention.
Berberine demonstrates some insulin-sensitizing effects comparable to metformin in multiple studies, as well as additional anti-inflammatory and lipid-lowering properties. It can be an option for women who prefer non-pharmaceutical approaches or who do not tolerate metformin.
GLP-1 receptor agonists, including tirzepatide at both therapeutic and microdose ranges, represent an increasingly important tool in PMOS management. Beyond weight regulation, GLP-1 agonists reduce systemic inflammation, improve insulin sensitivity, lower androgen levels, and appear to have direct beneficial effects on ovarian function. Their role in PMOS management is an active area of clinical research and growing clinical application.
Nutrition and lifestyle
A low-glycemic, anti-inflammatory dietary pattern consistently demonstrates benefit in PMOS, improving insulin sensitivity, reducing androgen levels, and lowering inflammatory markers. This does not require caloric restriction. It requires attention to carbohydrate quality, glycemic load, and the inflammatory burden of the overall dietary pattern.
Resistance training has specific and significant benefits in PMOS beyond general fitness. It improves insulin sensitivity through mechanisms independent of weight loss, increases SHBG, and supports the muscle mass that is metabolically protective over the lifespan. Aerobic exercise complements this through its anti-inflammatory and cortisol-regulating effects.
Sleep optimization is non-negotiable in a condition where sleep disruption directly worsens every metabolic driver of the syndrome. Screening for and treating sleep apnea where present is a therapeutic intervention, not a secondary concern.
HPA axis and stress physiology
Given the central role of HPA axis dysregulation in PMOS pathophysiology, interventions that support nervous system regulation and cortisol balance are clinically meaningful, not adjunctive. These include evidence-supported approaches to stress reduction, trauma-informed care where relevant, and adaptogenic support with compounds such as ashwagandha, which has documented cortisol-lowering and androgen-reducing effects in women.
Hormone optimization
For women with PMOS navigating perimenopause and menopause, the hormonal picture becomes more complex and requires individualized assessment. Estrogen decline compounds insulin resistance. Testosterone deficiency, which may coexist with the relative hyperandrogenism of PMOS, can worsen metabolic and cognitive outcomes. Progesterone has important insulin-sensitizing and cortisol-modulating effects. Thoughtful hormone optimization in this population requires understanding how the underlying PMOS physiology interacts with menopausal hormonal shifts.
Anti-androgen therapies, including spironolactone, address the symptomatic burden of hyperandrogenism, particularly for hair, skin, and hirsutism, but do not address the metabolic root causes and should be used within a comprehensive treatment framework rather than as standalone management.
Why the Rename Is a Beginning, Not an Ending
The renaming of PCOS to PMOS is a meaningful clinical and scientific correction. It accurately reflects that this is a polyendocrine and metabolic syndrome rather than a primary ovarian condition. It will influence how researchers frame their questions, how medical students are taught to recognize the condition, and how clinical guidelines are written.
But a name change does not automatically change culture. Women with PMOS have spent decades being referred in circles, dismissed when their labs did not fit the expected pattern, and treated for individual symptoms without anyone addressing the system generating them. The rename creates the conditions for better medicine. Whether better medicine actually follows depends on whether training changes, whether research funding shifts toward the metabolic and endocrine mechanisms that drive the syndrome, and whether physicians are willing to look at the whole body rather than the organ named in the diagnosis.
The body is an ecosystem. Hormones, metabolism, nervous system, inflammation, sleep, stress physiology, and lived experience are not separate clinical silos. They are one continuous, interconnected story.
Women with PMOS deserve care that reads that story from beginning to end.