
Low Testosterone in Women: What It Can Look Like and Why It Gets Missed.
Testosterone Is a Women's Hormone Too
She was 46 years old, still having regular periods, and convinced she was just getting old.
She had been doing CrossFit for years — the kind of woman who showed up at 6 am, who measured her recovery, who took her health seriously. But something had shifted. The workouts that used to feel strong now left her depleted for days. Her muscle mass was quietly disappearing despite training harder than ever. Brain fog had settled in like weather she couldn't clear. And her orgasms, when they happened at all, were shadows of what they used to be. Muted. Distant. Like trying to tune into a radio station that kept cutting out.
Sex had become painful. Not dramatically, not in a way that felt easy to name or explain to anyone, including her doctor. Just a creeping discomfort with penetration that made her dread something she used to enjoy. She was in a long-term marriage, and they often struggled sexually to connect, so she just chalked it up to that. But her body simply wasn't responding the same way it once had.
She wasn't depressed. She wasn't burned out (yet). She was, by every external measure, healthy.
Her labs told a different story.
Her testosterone was far below the normal range. Not borderline or slightly below range, but genuinely depleted. What made it more interesting was her history: she had been on hormonal birth control for years before her tubal ligation twelve years earlier, and birth control pills are well documented to suppress testosterone production and increase sex hormone binding globulin, which binds up whatever free testosterone remains. She had experienced severe pain with sex back then, but that had improved when she went off the pill nearly a decade ago. But her testosterone had never fully recovered.
She started a compounded testosterone formula in liquid drops, applied to her wrist every morning. No patch. No injection. No mess. A small, precise, adjustable dose that could be titrated as her body responded.
Within weeks, the brain fog began to lift. Within months, her workouts felt like her workouts again. The pain with sex gradually resolved. And her orgasms came back, not as echoes, but as the full, embodied experience she had almost forgotten was possible.
That woman was me.
I share this not because my story is unusual, but because it isn't. Versions of this walk into my office regularly. And the women living inside them have almost never been told that testosterone could be part of what's missing.
What We Were Never Taught About Testosterone
For decades, women have been told testosterone is a male hormone. That framing is not only inaccurate but outright false, and it has caused real harm. Women produce testosterone throughout their lives, primarily in the ovaries and adrenal glands. In fact, women produce more testosterone than estrogen. We simply have fewer androgen receptors available in our cell membranes to use it, which is why the conversation around levels requires nuance rather than simple comparison to male ranges.
Testosterone influences sexual desire and arousal, energy, motivation, confidence, muscle strength and maintenance, bone density, cognitive function, and emotional resilience. It is not a secondary hormone in the female body. It is a foundational one.
In perimenopause and menopause, testosterone often declines alongside estrogen and progesterone. Some women notice this as a sudden shift. Others experience it as a gradual dimming of vitality that is difficult to name but impossible to ignore. This is one reason why hormone conversations focused exclusively on estrogen so often leave women feeling like something is still missing.
What Low Testosterone Actually Looks Like
Low testosterone in women rarely announces itself with a clear label. It tends to look like fatigue that sleep doesn't fix, motivation that quietly disappeared, brain fog that makes sharp women feel suddenly dull, reduced muscle mass despite consistent exercise, poor recovery from physical exertion, emotional flatness, and a loss of the confidence and aliveness that used to feel natural.
It frequently looks like low libido. But libido is more complex than simple sex drive. Desire lives in the brain, the nervous system, sleep quality, stress load, body image, emotional safety, and relational dynamics, not just hormone levels. Testosterone affects all of these systems simultaneously, which is why its decline can feel so diffuse and hard to trace.
Many women describe feeling less spontaneous desire, less responsive to touch, reduced orgasm intensity, or a quiet disconnection from their own sexuality that they can't quite explain. When testosterone is appropriately replaced in carefully selected patients, many report not just improved desire and arousal but a broader sense of aliveness, embodiment, and energy that they had stopped expecting to feel again.
These symptoms also overlap significantly with thyroid dysfunction, insulin resistance, chronic stress, burnout, poor sleep, and medication side effects, which is exactly why individualized evaluation matters rather than treating a number on a lab panel in isolation.
What Testosterone Does in Vulvar and Vestibular Tissue
This is the part of the testosterone conversation that almost never gets discussed, even in medical settings, and it is critically important.
The vulva, vestibule, vaginal walls, and urethra are all androgen-sensitive tissues. Embyologically, all humans derive from similar structures, but the androgen receptors in male DNA form the penis and testicles.
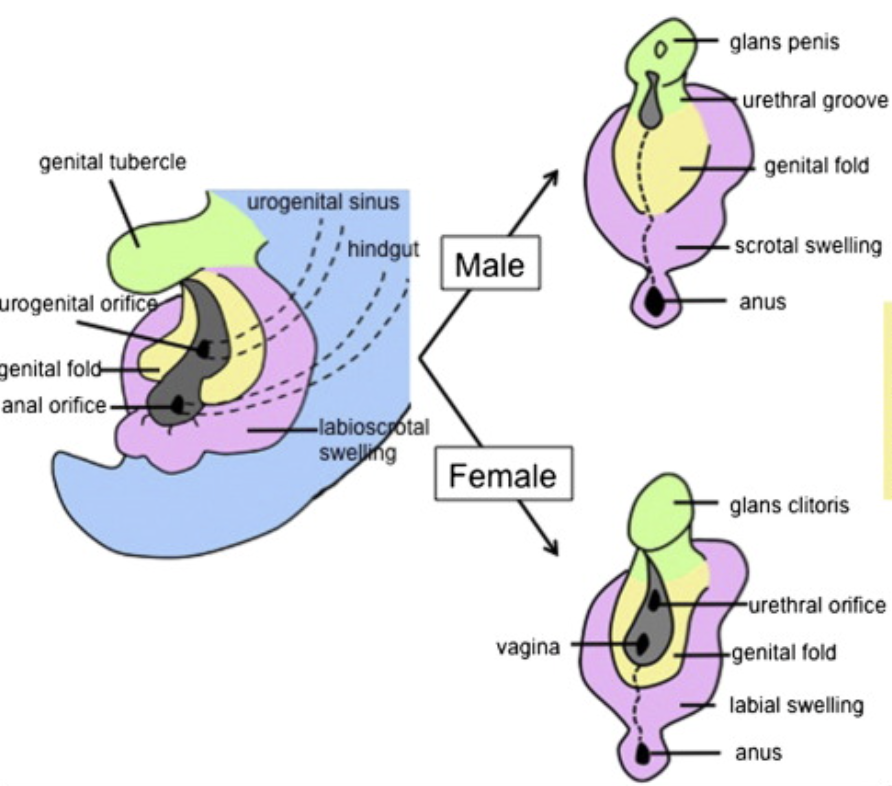
Androgens and mammalian male reproductive tract development.
Aki Murashima, Satoshi Kishigami, Axel Thomson, Gen Yamada, Androgens and mammalian male reproductive tract development, Biochimica et Biophysica Acta (BBA) - Gene Regulatory Mechanisms, Volume 1849, Issue 2, 2015, Pages 163-170,SSN 1874-9399
The female urethra and vestibular tissues contain androgen receptors that depend on testosterone for their health, thickness, elasticity, lubrication, and nerve function. When testosterone declines, these tissues don't just lose estrogen support. They also lose androgen support, and the effects are distinct and significant.
Low testosterone in vulvovaginal tissues contributes to thinning of the vestibular tissue, which is the delicate area at the vaginal opening. This thinning leads to increased sensitivity to pain, reduced natural lubrication, decreased tissue elasticity, and the kind of burning and discomfort with penetration that women often describe as feeling like tearing or rawness, even with adequate arousal.
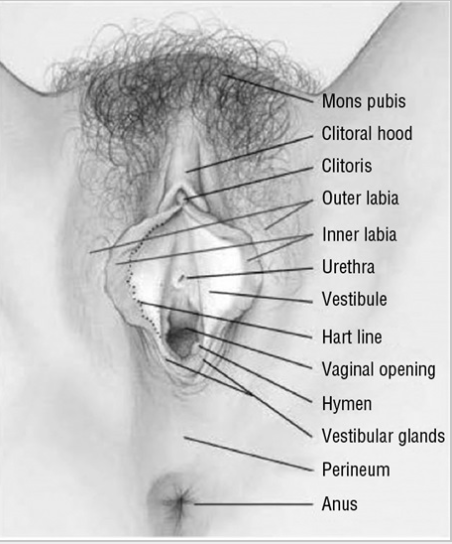
Vulva anatomy. The vulva consists of the organs immediately external to the vagina: mons pubis; clitoris; labia majora; labia minora; vulvar vestibule; urethral meatus; hymen; Bartholin and Skene glands and ducts; and vaginal introitus. Image courtesy of Dawn Danby and Paul Waggoner, co/ the International Society for the Study of Vulvovaginal Disease. Reprinted from International Society for the Study of Vulvovaginal Disease. The normal vulva. Waxhaw [NC]: ISSVD; 2013.
This is closely connected to Genitourinary Syndrome of Menopause, known as GSM, a condition that includes vaginal dryness, pain with penetration, burning, urinary urgency, and recurrent urinary tract infections. GSM has traditionally been treated with vaginal estrogen alone, which absolutely helps. But for many women, estrogen alone is not sufficient because the androgen receptor component of the tissue's health has been left unaddressed.
The urethra is particularly rich in androgen receptors and shares embryological origins with male urethral tissue (see image above comparing them). When testosterone declines, urethral tissue loses thickness, resilience, and nerve sensitivity. The protective lining becomes more fragile, the local microbiome shifts, and bacteria find it easier to colonize. This is one of the underrecognized reasons why recurrent UTIs become more common in perimenopausal and menopausal women, and why some women respond only partially to vaginal estrogen but dramatically improve when local or systemic testosterone is added.
Pain with penetration, often diagnosed broadly as dyspareunia or vulvodynia, frequently has a testosterone deficiency component that is missed when providers look only at estrogen levels and vaginal pH. The vestibular tissue requires androgenic support to maintain its nerve function and pain threshold. Without it, even gentle contact can become acutely uncomfortable.
This was part of my own story. The pain I was experiencing wasn't simply dryness. It was tissue that had lost its androgenic foundation, even at 43, even with regular cycles, even years after stopping the hormonal contraception that had set the deficit in motion.
The Birth Control Connection
This deserves its own conversation.
Hormonal contraceptives, particularly combined oral contraceptives, suppress ovarian testosterone production and significantly elevate sex hormone binding globulin (SHBG), a protein that binds testosterone and renders it biologically unavailable. The result is a reduction in both total and free testosterone that can be substantial.
For many women, testosterone levels recover after stopping hormonal contraception. For others, SHBG remains persistently elevated and free testosterone remains suppressed for years, sometimes indefinitely. This means a woman can be off the pill for eight years, as I was, and still be carrying the hormonal aftermath of years of suppression.
This is not discussed when contraception is prescribed. Women are not warned that a side effect of hormonal birth control may be a lasting alteration in their hormonal baseline, with downstream effects on desire, sensation, tissue health, and pain. They deserve to know this.
A Note on Pellet Therapy
Because testosterone has become increasingly visible in women's wellness conversations, pellet therapy has expanded aggressively into this space, marketed as natural, effortless, and life-changing.
The problem is that pellets deliver large, fixed doses of testosterone that cannot be adjusted once inserted. If a woman develops side effects including acne, scalp hair loss, irritability, anxiety, voice changes, or testosterone levels that climb far above physiologic female ranges, the medication cannot simply be stopped. It continues releasing for months regardless of how the patient responds.
This is not precision medicine. It is not personalized care. And the financial incentive structure built around repeat insertions, with minimal attention to comprehensive evaluation, is something I find genuinely concerning.
The approach I use for testosterone therapy, including my own, is compounded transdermal drops or creams that allow for careful titration, easy dose adjustment, and the ability to stop or modify treatment quickly if needed. The goal is always restoration to physiologic levels that support function and quality of life, not supraphysiologic levels that create new problems.
On the Fear of Becoming Masculine
This comes up in nearly every conversation I have about testosterone therapy with women, and it deserves a clear answer.
Physiologic testosterone replacement does not make women aggressive, emotionally numb, or less feminine. It does not masculinize. What it does is restore the hormonal foundation that supports vitality, embodiment, and aliveness in the female body.
Many women describe feeling more themselves on appropriate testosterone therapy, not a different version of themselves, but a clearer, more energized, more present version of the woman they already are. More confident. More in their body. More able to access pleasure without the interference of fatigue, flatness, and physical discomfort.
That is not masculinization. That is restoration.
Why This Goes Undiagnosed
Women's medicine has historically minimized symptoms that cannot be resolved with a quick procedure or a clear diagnostic category. Fatigue, loss of desire, brain fog, emotional flattening, pain that doesn't fit neatly into a diagnosis: these are regularly attributed to stress, aging, depression, or the demands of modern life.
But common does not mean acceptable. And a symptom being difficult to measure does not make it less real.
Women who present with the constellation I've described, diminished orgasm, pain with penetration, exercise intolerance, brain fog, and emotional flatness, are far more likely to be offered antidepressants than a testosterone panel. The conversation they deserve, an honest, individualized evaluation of their full hormonal picture including androgens, rarely happens.
That is a failure of medicine. Not a failure of the women sitting in the exam room.
Is Testosterone Right for You?
Not for everyone, and it is not a magic fix for anything. It is one important tool within a larger framework of care that also addresses sleep, stress physiology, metabolic health, relationship dynamics, medications, nutrition, pelvic floor health, and genitourinary tissue health.
But if you are in your 40s with regular cycles and feel like your body has quietly stopped responding the way it used to, if orgasms have become elusive, if sex has become uncomfortable, if the workouts that used to restore you now deplete you, if you feel like a dimmer and more distant version of yourself, testosterone may be part of the picture that no one has thought to look at yet.
I know this because I lived it.
I apply my drops to my wrist every morning. It takes seconds. The dose is precise and adjustable. There is no mess, no injection, no pellet I cannot take back if something shifts.
And I feel like myself again.
That is what this work is for. Not chasing youth. Not optimizing performance. Just helping women feel fully alive in the bodies they are living in right now, with the honesty, evidence, and individualized care that has always been their due.
Because feeling alive in your body matters. And you deserve a doctor who agrees.