
Recurrent UTIs in Women: Why Hormones Matter More Than You've Been Told
She came in carrying a list of every UTI she'd had in the past two years. Seven infections. Seven courses of antibiotics. Seven temporary reprieves followed by the same burning, urgency, and defeat.
She had followed every rule she'd ever been given. She peed after sex. She wiped correctly. She avoided hot tubs and bubble baths and everything else on the list her previous doctor had handed her like a permission slip for shame. She was doing everything right and still couldn't stay well.
What nobody had ever checked was actually examining her vulvar tissue, accounting for her hormone status, and getting a history of oral contraceptive pill use. While this can be a telltale sign of genitourinary syndrome of menopause, it can also occur years before menopause occurs.
This is one of the most common and most preventable failures I see in women's medicine. Recurrent urinary tract infections in women are NOT a hygiene problem, more often than not an anatomy problem, and not bad luck. They are often a hormone problem. And until we address the tissue environment that makes women vulnerable to these infections in the first place, we are simply chasing bacteria while the real issue goes untreated.
What Hormones Have to Do With Your Bladder
The urinary system is hormone-sensitive tissue. Most people don't know this. Most physicians don't discuss it.
Estrogen plays a foundational role in maintaining the health of the bladder, urethra, vagina, and vulva. It supports blood flow, collagen production, tissue elasticity, natural lubrication, vaginal pH, and the protective lactobacilli that keep the vaginal microbiome balanced and hostile to bacterial overgrowth. When estrogen declines during perimenopause and menopause, every one of those protective mechanisms weakens simultaneously. The tissue becomes thinner, drier, more fragile, and far more susceptible to colonization by the bacteria responsible for UTIs.
But estrogen is only part of the story, and this is where the conversation almost always stops too soon.
The female urethra is rich in androgen (testosterone)receptors. Structurally and embryologically, it shares significant similarities with male urethral tissue and depends on testosterone to maintain its thickness, blood flow, nerve sensitivity, and resilience. When testosterone declines, as it often does in perimenopause before estrogen does, the urethral lining becomes more fragile, the local microbiome shifts, and bacteria find it significantly easier to colonize.
This is why some women respond only partially to vaginal estrogen and dramatically improve when testosterone is added. The tissue has androgen receptors that estrogen alone cannot address. For these women, a compounded estradiol and testosterone cream applied locally to the vulvar and urethral tissues can be genuinely transformative, not because it is experimental, but because it is treating the actual physiology rather than the symptom.
This isn't simply aging. This is physiology. And physiology can be supported.
The Antibiotic Trap
Antibiotics are sometimes necessary and genuinely helpful. I am not suggesting otherwise. But many women find themselves in a cycle that goes: infection, antibiotic, temporary relief, recurrence, another antibiotic, and around again, while the underlying tissue vulnerability that is driving the infections goes completely unaddressed.
Repeated antibiotic courses carry real consequences beyond the inconvenience of taking them. Antibiotic resistance is a growing clinical problem. Microbiome disruption leads to yeast overgrowth and gastrointestinal side effects. And because antibiotics do nothing to restore the tissue environment that enabled the infection, the bacteria simply return to a host that remains vulnerable.
When infections keep coming back shortly after treatment ends, that is not a sign that you need a stronger antibiotic. It is a signal that something deeper needs attention.
What Actually Helps
The single biggest clinical game-changer I see in practice is local hormone therapy. Low-dose vaginal estrogen has strong, consistent evidence supporting its use in postmenopausal women with recurrent UTIs. Studies show significant reductions in infection rates when it is used regularly, and it comes in several forms, including creams, inserts, tablets, and rings. The goal is not symptom management. It is a genuine restoration of tissue health.
An underused option that more women deserve to know about is prasterone, sold under the brand name Intrarosa, or can be compounded as a cream or suppository. This is vaginal DHEA, a precursor hormone that tissues can locally convert into both estrogen and testosterone, depending on their specific needs. Rather than delivering hormones systemically, it works at the tissue level to improve integrity, lubrication, resilience, and urinary health. Emerging research suggests women using vaginal DHEA have meaningfully lower rates of recurrent UTIs, likely because it supports both the estrogen and androgen pathways within the tissue itself.
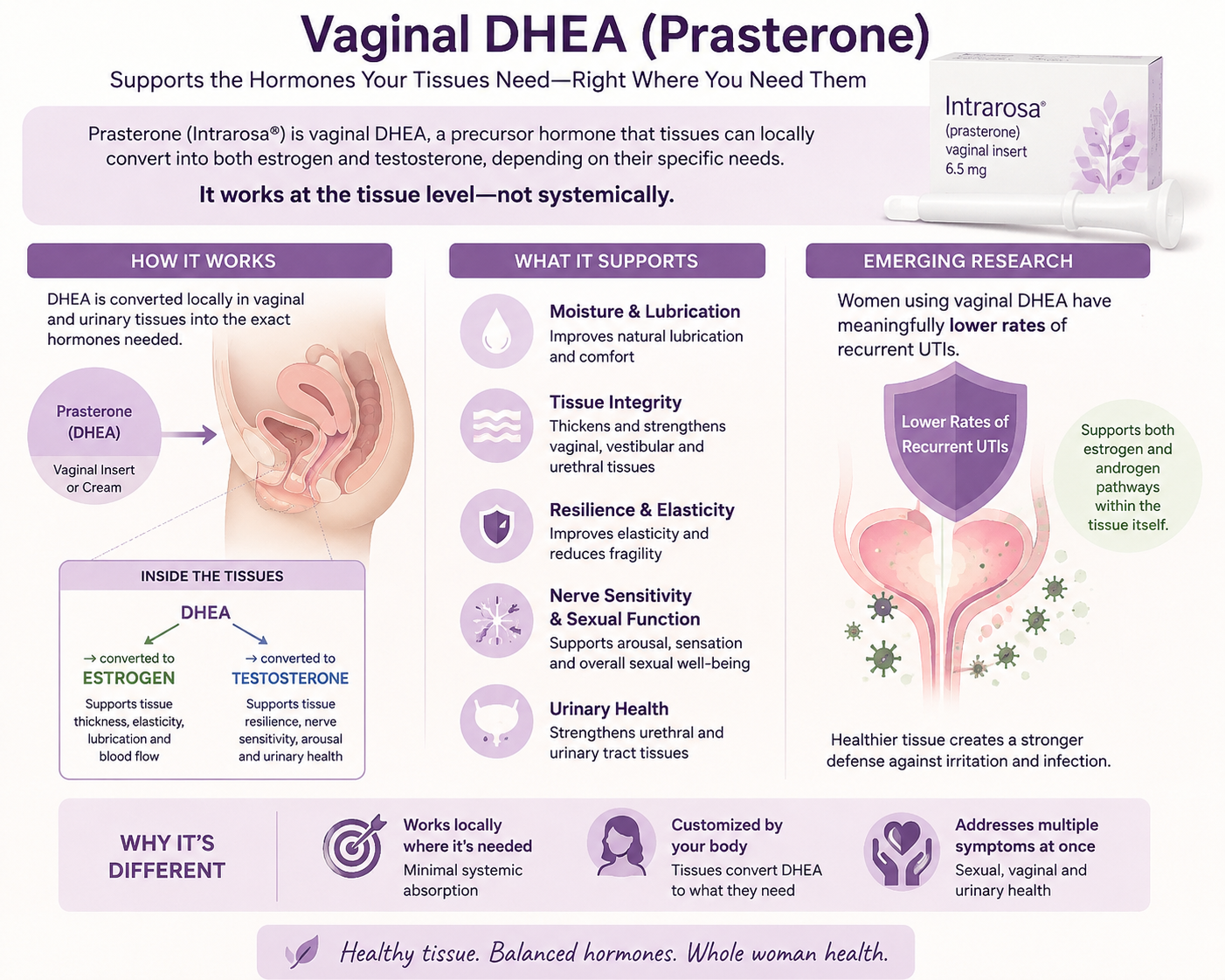
Medical infographic explaining how vaginal DHEA, also called prasterone or Intrarosa, is locally converted into estrogen and testosterone within vaginal and urinary tissues to improve lubrication, tissue integrity, sexual function, resilience, and urinary health while reducing recurrent UTIs
Created by ChatGPT and reviewed by Dr. Dacker
Simple hydration matters more than most women realize. Increasing daily water intake appears to reduce recurrent infections consistently across studies. And spermicides are worth avoiding entirely because they disrupt the vaginal microbiome and meaningfully increase infection risk, yet this is rarely discussed.
On the Supplements Everyone Is Talking About
D-mannose became enormously popular online as a UTI-prevention tool, and its appeal is understandable. However, recent randomized controlled trials have produced disappointing results compared with placebo. The evidence simply does not support the enthusiasm.
Probiotics follow a similar pattern. The concept makes biological sense, but the evidence remains inconsistent, and the product quality varies so dramatically that making reliable recommendations is genuinely difficult. We are not there yet with probiotics for UTI prevention.
Cranberry products, somewhat surprisingly, have better evidence than most people expect. The active compounds, called proanthocyanidins, or PACs, appear to interfere with bacteria adhering to the bladder wall. What matters is dosage. Products containing at least 36 mg of PACs daily appear to offer the most meaningful benefit, and the majority of cranberry supplements on the market do not meet that threshold. Read the label before you buy.
One of the most underused and underknown tools in my practice is methenamine hippurate. This is not an antibiotic. It converts into formaldehyde within acidic urine and suppresses bacterial growth without contributing to antibiotic resistance. Recent studies found it performed comparably to preventive antibiotic regimens for recurrent UTIs while avoiding the long-term microbiome and resistance concerns that come with chronic antibiotic use. It is an option that far more women and far more physicians should know exists.
Treating the Tissue, Not Just the Infection
What frustrates me most about how recurrent UTIs are managed in women's medicine is not the gaps in knowledge. It is the blame.
Women are handed hygiene checklists and sent home with antibiotics while the hormonal, vascular, and tissue changes that are actually driving their infections go entirely unexamined. The implicit message is that recurrent UTIs are something a woman is doing wrong. That she is somehow responsible for failing to prevent an infection in tissue that has been quietly losing its protective architecture for years.
Recurrent UTIs are not a hygiene failure. They are frequently a failure of the tissue environment. And when we start treating the environment rather than endlessly chasing individual infections, outcomes improve in ways that feel, to the women experiencing them, like nothing short of revelatory.
You deserve a more thoughtful conversation than another antibiotic and another list of rules. You deserve medicine that understands the bladder, the urethra, the vagina, the hormones, the nervous system, and the microbiome as the deeply interconnected systems they actually are.
Because treating the root cause is a fundamentally different thing from managing symptoms indefinitely.
And you have been managing symptoms long enough.
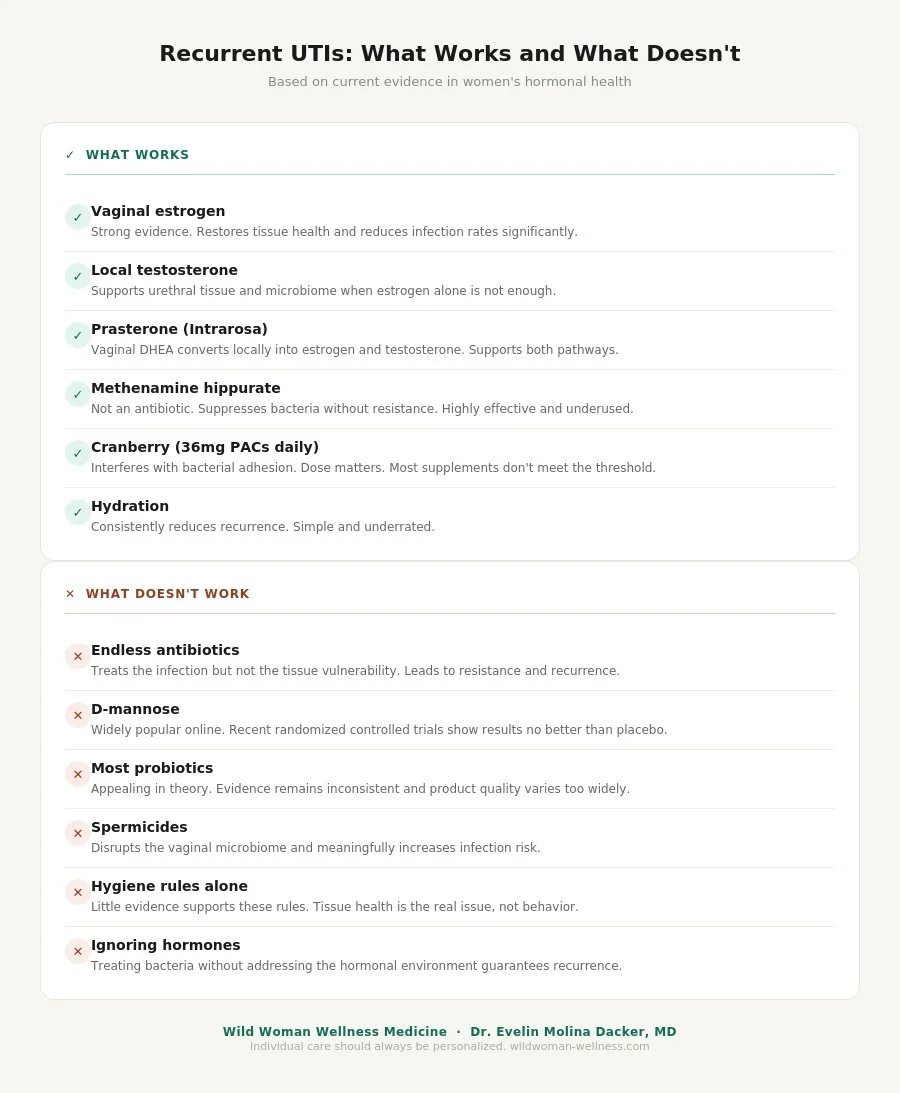
Recurrent UTIs: What Works and What Doesn't" by Dr. Evelin Molina Dacker, MD of Wild Woman Wellness Medicine. The left column lists six evidence-based treatments that work, including vaginal estrogen, local testosterone, prasterone, methenamine hippurate, cranberry at 36mg PACs daily, and hydration. The right column lists six approaches that do not work, including endless antibiotics, D-mannose, most probiotics, spermicides, hygiene rules alone, and ignoring hormones. Each item includes a brief clinical explanation.