
GLP-1 Medications for Weight Loss: What GLP-1 Medications Are Actually Doing in the Body
There’s a massive shift happening in medicine right now around weight, metabolism, and how we understand obesity.
And honestly? Most conversations about GLP-1 medications are still incredibly oversimplified.
People talk about these medications as if they are just “appetite suppressants” or a shortcut to weight loss. But that misses the deeper physiology entirely. These medications act on complex hormonal systems that influence the brain, pancreas, liver, stomach, fat tissue, metabolism, and energy expenditure simultaneously.
This is why they can feel so different from traditional dieting.
And this is also why the newer medications are becoming increasingly powerful.
To understand the difference between semaglutide, tirzepatide, survodutide, and retatrutide, you first have to understand the hormones they mimic.
GLP-1: “Stop Eating, Slow Things Down”
GLP-1 stands for glucagon-like peptide-1. It’s part of the incretin system, a network of gut hormones released when you eat. Your body naturally produces GLP-1 in response to nutrients entering the small intestine. This is Semaglutide, brand name Ozempic (diabetes) and Wegovy (weight loss).
GLP-1 does several important things simultaneously.
First, it helps the pancreas release insulin, but only when glucose is present. This is important because it lowers the risk of hypoglycemia. Your body isn’t just dumping insulin indiscriminately. It’s responding intelligently to food intake.
Second, GLP-1 suppresses glucagon, the hormone that raises blood sugar. This helps stabilize glucose levels after meals.
Third, it slows gastric emptying. Food stays in the stomach longer, which reduces blood sugar spikes and increases fullness.
But clinically, the most fascinating effect may be what GLP-1 does in the brain.
GLP-1 changes appetite signaling and food reward pathways. Many people describe this as a reduction in “food noise.” They stop thinking about food constantly. Cravings quiet down. Satiety becomes easier to access.
This is why semaglutide, the first-generation GLP-1 medication, was such a major breakthrough.
Not because it simply made people eat less, but because it altered the biological systems driving hunger and reward in the first place.
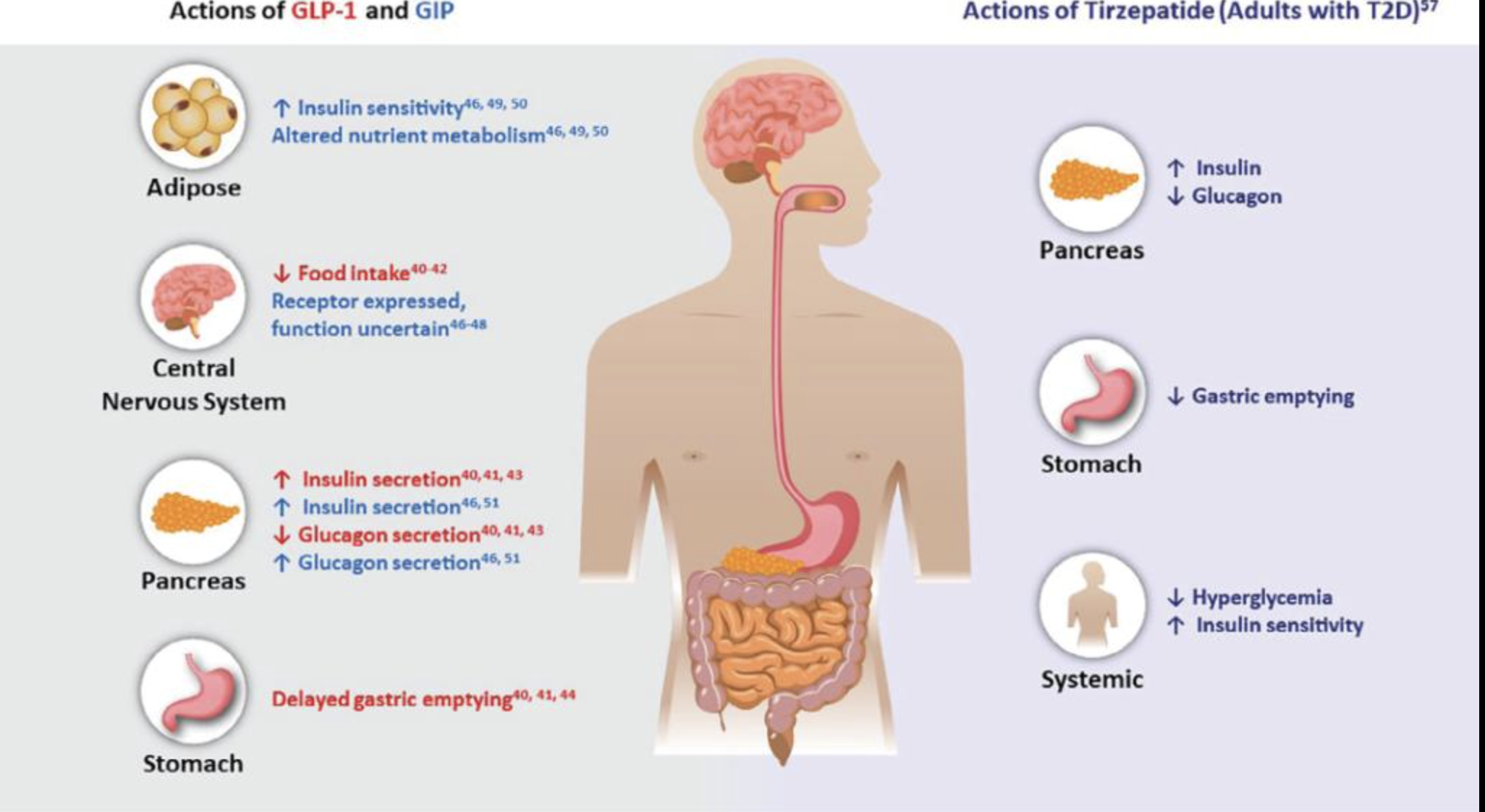
Medical illustration showing how GLP-1 and GIP medications like tirzepatide affect the brain, pancreas, stomach, adipose tissue, insulin sensitivity, glucagon levels, gastric emptying, and appetite regulation in the body
GIP: “Handle Incoming Nutrients Efficiently”
The next evolution came with GIP, glucose-dependent insulinotropic polypeptide. This is Tirzepatide, brand name Mounjaro (diabetes) and Zepbound (weight loss).
Like GLP-1, GIP is part of the incretin system and is released when you eat, especially in response to carbohydrates and fats. But GIP appears to play a slightly different role.
Where GLP-1 says, “Slow down and stop eating,” GIP seems to help the body manage and utilize incoming nutrients more efficiently.
GIP enhances insulin release in the presence of glucose and acts synergistically with GLP-1. Together, these hormones improve blood sugar control, regulate appetite, and influence how fuel is processed and stored.
Interestingly, GIP on its own may promote fat storage under normal physiologic conditions. But when paired with GLP-1 in medications like tirzepatide, the overall effect appears very different.
Tirzepatide improves insulin sensitivity, enhances metabolic efficiency, and may reduce some of the gastrointestinal side effects commonly seen with GLP-1 medications alone. This is one reason many people experience greater weight loss and improved tolerability with tirzepatide compared to earlier GLP-1 medications.
Glucagon: “Release Stored Energy”
Then comes the hormone most people are surprised to hear about in obesity treatment: glucagon.
Traditionally, glucagon has been thought of as the hormone that raises blood sugar. It’s released by the pancreas when blood sugar drops or when the body needs fuel between meals.
Glucagon tells the liver to release stored glucose and create new glucose. It also shifts the body into a fuel-mobilizing state by increasing fat breakdown and ketone production.
But glucagon does something else important.
It increases energy expenditure.
In other words, it may help the body burn more fuel.
This is where medications like survodutide and retatrutide become especially interesting. These medications have not been officially FDA-approved, but will be on the market soon.
When glucagon activity is carefully balanced with GLP-1, you may get both decreased appetite and increased energy expenditure simultaneously. The body is not only taking in less fuel, but it is also potentially burning more.
This represents a major shift in obesity medicine.
For decades, obesity treatment has largely focused on restriction and willpower. But newer research increasingly recognizes obesity as a metabolic and neurohormonal condition involving energy regulation, reward systems, insulin signaling, inflammation, and fuel utilization.
The Evolution of These Medications
Each generation of medication builds on these hormonal systems in slightly different ways.
Semaglutide primarily works through GLP-1 pathways, slowing digestion, increasing fullness, and reducing appetite.
Tirzepatide combines GLP-1 and GIP, improving metabolic regulation and nutrient handling.
Survodutide combines GLP-1 with glucagon activity, potentially increasing fat burning and energy expenditure.
Retatrutide combines GLP-1, GIP, and glucagon, creating a broader metabolic effect that may influence appetite, insulin sensitivity, and energy burning all at once.
Some of these medications are still under investigation and not yet FDA approved.
But None of This Bypasses Human Physiology
This is the part I think is often missing online.
These medications can be incredibly helpful tools. For some people, they are life-changing. They may reduce inflammation, improve insulin resistance, decrease cardiovascular risk, quiet compulsive eating patterns, and support significant weight loss.
But they are not magic.
Long-term metabolic health still depends on foundational physiology:
Sleep, muscle mass, nutrition, stress regulation, hormones, movement, and nervous system health!
This is also why some people lose weight on these medications but still do not feel well. Or lose muscle mass. Or regain weight when stopping them without deeper lifestyle support.
The goal should never just be smaller bodies.
The goal is healthier metabolism, preserved muscle, improved energy, reduced disease risk, and a more sustainable relationship with your body.